Red flags
Red flags are signs and symptoms that refer to sinister or serious medical conditions requiring urgent, specific medical intervention. These include malignancy, inflammatory disorders, fracture, infection, and cauda equina syndrome. These conditions only make up a tiny percentage (~1-3%) of people presenting to primary care. Nevertheless, as they have serious consequences when left unaddressed, they must be screened for with care.
It’s accepted that red flags are not an exact science and some value is given to “gut feeling” when being assessed. However, many physios do not remain sensitive to the presence of red flags in their assessment! A personal friend of mine did not receive the care he needed because the physio he was being treated by missed important (and dare I say obvious!) red flags. Unfortunately my friend passed away; perhaps this could have been different if he was initially assessed well?
This list below does not replace face-to-face medical assessment.
Rather than being a rule book, this list serves as a guide to aid recognition of red flags for those in pain.
- Loss of feeling/pins and needles/numbness between the inner thighs, genitals, in or around the back passage or buttocks
- Not knowing when bladder is full or empty or increasing difficulty in urinating/controlling flow/stopping urinating or loss of sensation when passing urine
- Change in ability to achieve an erection or ejaculate or loss of genital sensation during intercourse
- New onset/progressively worsening muscle weakness
- Persistent, and worsening non-mechanical pain, including severe night pain
- Mechanical symptoms non-responsive to appropriate management over a reasonable time scale (~3 months)
- Unwell/fever/night sweats
- Recent unexplained weight loss
Finally, there are also site-specific red flags that relate to various body parts that also need medical evaluation. Click here for more info regarding specific low back pain red flags. Also please see the Australian Acute Musculoskeletal Pain Guidelines (2004) and Ross and Boissonnault (2010) for a more comprehensive documentation of the subject.
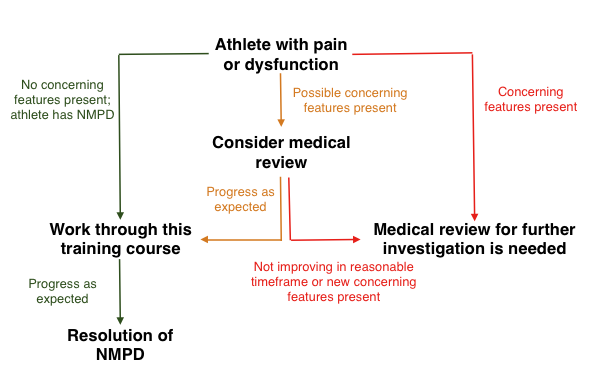
Adapted from International Framework for Red Flags and serious spinal pathologies published in JOSPT. ‘[T]his training course’ refers to the Abound Online | Physio In Your Pocket found here. ‘NMPD’ stands for non-sinister musculoskeletal pain disorder.
Specific diagnosis
A specific musculoskeletal pain disorder (MPD) refers to a disorder of the musculoskeletal system that accounts (at least in part) to an individual’s pain or symptoms. For example, specific MPDs could include:
- Rheumatoid arthritis
- Stress fracture
- Ruptured tendon
- Protruded disc with associated radiculopathy (pain/weakness/altered sensation anywhere along the part of the body served by that compressed nerve)
Sometimes resolution of the specific diagnosis will result in resolution of the MPD and sometimes it won’t. Sometimes addressing other components (e.g., lifestyle factors [poor sleep, doing too much exercise too quickly etc.] or psychosocial factors [work-related stress, lack of meaningful activities etc.]) can resolve the pain.
A combination approach (ie., shotgun, rather than sniper) is best as:
- we can’t know for sure what’s needed to recover, and
- there’s always influence between the various factors (for good or bad).
Non-specific diagnosis
Structural or pathoanatomical diagnoses can often be over-emphasised, and may not be as important as we once thought for management of non-sinister musculoskeletal pain disorders (NMPDs) given that,
- extremely large differences exist between individuals (strength, ROM, body proportions, etc.),
- special tests done by physios aren’t that special (ie., in general they lack specificity and sensitivity (e.g., Hadedus 2012),
- there’s very poor correlation between what we find on scans and someone’s pain/dysfunction (e.g., Brinjikji et al., 2015),
- and perhaps most importantly, pathoanatomical diagnoses rarely meaningfully change management on non-sinister problems.
If red flags are not present and the athlete does not have a specific diagnosis (or if the specific diagnosis is deemed irrelevant to the MPD), then a ‘non-specific diagnosis’ label can be used.
Diagnoses rarely meaningfully change management of non-sinister pain!
A non-specific diagnosis will likely be utilised in >90% of all MPDs – and this is totally fine! It simply means,
- you don’t have anything serious going on,
- a specific diagnosis won’t meaningfully change management,
- a specific diagnosis cannot be known,
- and/or an unhelpful and overly biological/ structural view of the body will not be pursued
So, if you have a non-specific diagnosis, be reassured and encouraged! Individuals with non-specific diagnoses can, of course, utilise Abound Online programmes found here.
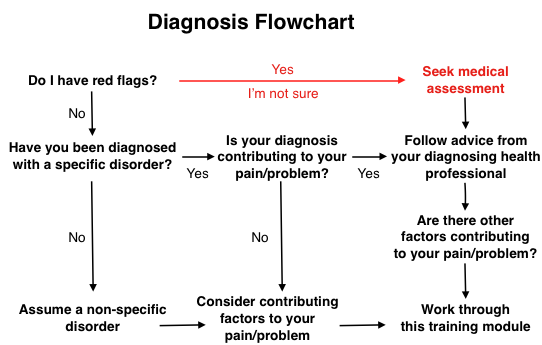
The Diagnosis Flowchart. ‘This training module’ refers to the Abound Online Programs found here.
Thanks for reading!
For thorough assessment and treatment book in! We’d love to help you navigate your low back pain!
